follow up for colonoscopy after polypectomy
Adenomatous colon polyps are considered to have malignant potential. Although not all adenomatous polyps will become malignant, they may demonstrate a typical progression from dysplasia to carcinoma in situ and finally adenocarcinoma. Patients at average risk are advised to undergo screening colonoscopy at 10-year intervals, but patients with adenomatous polyps are at increased risk for future colon cancer and require more frequent follow-up colonoscopy.
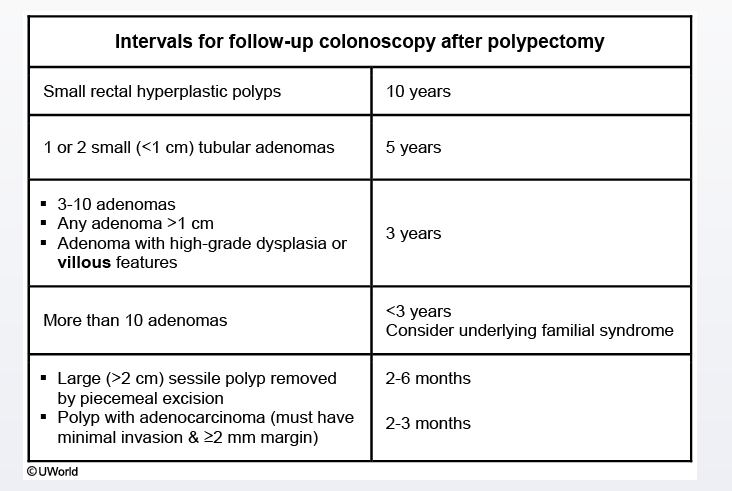
Management of adenocarcinoma arising in a polyp is dependent on its pathologic features. Most cases of adenocarcinoma require surgical resection. However, if the invasive adenocarcinoma is in the head of the polyp, the margins are uninvolved (>2 mm), the lesion is well-differentiated, and there is no lymphovascular invasion, the patient can usually undergo nonoperative management. Patients should be advised of treatment recommendations after careful consultation on a case-by-case basis. In patients who are managed nonoperatively, follow-up colonoscopy should be performed in 2-3 months to exclude residual or recurrent disease. This short-interval follow-up can also assess for a synchronous lesion that may have been missed. The endoscopist can tattoo the area of the polyp at the time of initial biopsy so that the area can be found easily in the future. Subsequent follow-ups should be obtained 1, 4, and 9 years following the initial polyp resection.